
Professor Gordon Dougan FRS
The United Kingdom lost most of its vaccine manufacturing capacity in the 1980s. I was there and saw it happen. COVID-19 has shown how vital vaccine knowhow and production capacity is for any country and region. Here is my personal perspective on what is needed to build towards a more equitable vaccine world.
Up until the late 1970s, the United Kingdom had a thriving vaccine industry with global reach and innovative science based around two companies: The Wellcome Foundation* and Glaxo. Both companies were involved in vaccine discovery, development, and manufacturing. The UK’s manufacturing capacity was significant and could easily supply the nation’s human and animal vaccine requirements and, in addition, sell these products globally. This UK technology and expertise had grown over a 70-year period, through manufacturing and selling vaccines such as polio, tetanus and whooping cough. These companies provided extensive national knowhow and consumer confidence. Furthermore, vaccines were sold alongside complementary diagnostics and other reagents for the research community. During this time, many countries operated their own independent national vaccine supply organisations.

However, in the 1980s, events began to erode the UK-based vaccine industry and the diversity of vaccine manufacturing globally. In the decades before 1980, vaccines and other public health initiatives had driven down the incidence of infectious diseases in the richer economies and profits began to dwindle in this therapeutic domain. Also, innovation in the vaccine world had started to stagnate, although ironically enormous opportunities were just around the corner created by upcoming discoveries in recombinant DNA, monoclonal antibodies and genomics (1).
After 1980, more and more vaccine producers across the world started to close their doors or were bought by large companies. This was a period of consolidation. Single country manufacturers could not compete economically and lacked investment. Throughout this period, management discussions in pharmaceutical companies focused on the poor profitability of the vaccine business in comparison to other therapeutic areas. Vaccines were performing their role too well, having controlled many infections in the UK and similar economically developed countries. Additionally, few new vaccines had originated from the UK and the whole area became under-valued. Attitudes were also changing in the global business world as privatisation, merger and profit began to dominate.
From the 1930s, The Wellcome Foundation had been entirely owned by The Wellcome Trust. This provided a unique operational environment, with the only shareholder being a charity with a mission of improving scientific research. However, as the 1980s progressed, parts of the company were sold off or privatised leading to a change in attitude and the eventual acquisition of the company by Glaxo in 1995.
The Board of The Wellcome Foundation made the first move to exit the vaccine business by divesting their animal vaccines into a joint company with ICI Zeneca (now part of AstraZeneca), called Coopers Animal Health. This was at the same time as their scientists were making huge progress towards developing new animal vaccines. For example, with collaborators they solved the atomic structure of the Foot and Mouth Disease virus, opening the way for a subunit vaccine (2).
Soon after selling off the veterinary vaccine business the Wellcome Foundation Board made the decision to divest their human vaccine programme. This was one of the biggest decisions in the history of the company and was to have a profound impact on the future of vaccine research and manufacturing in the UK. The human vaccine arm was bought by venture investors who owned a company called Medeva (3). Medeva continued to make Wellcome vaccines, transferring some of the production team to Speke near Liverpool. We (see below) negotiated with Medeva to fund a small vaccine research arm, which we established at Imperial College London. Medeva eventually went through a series of acquisitions and the vaccine business was largely lost to the UK, apart from the production arm in Speke, which still make flu vaccines (https://www.seqirus.com/our-company, owned by the parent Australian company, CSL).
My experience
I am one of a dwindling group of people who worked in the UK vaccine industry in the heydays. Working at The Wellcome Foundation in Beckenham, I ran a research team focusing on bacterial vaccine development; my laboratory was located directly above vaccine scale up, manufacturing and quality assurance facilities. Thus, all the steps to discovering and manufacturing vaccines were on a single site. This provided a perfect setting to take vaccines from discovery right through to licensure. The company had a significant investment in research working on vaccines including malaria, whooping cough, Hepatitis B and Meningitis. Indeed, one of the first malaria vaccine candidates, antigen MSP1, was discovered in their laboratories (4). The companies research was indeed strong. During my ten years at the company, their scientists were awarded four Nobel Prizes (Vane, Elion, Hitchin, Black), quite remarkable (5).
In contrast to the research science base, the development and marketing side for vaccines was neglected and became weakened. This meant that many good ideas struggled to move forward against internal competition from products such as the then novel humanised monoclonal antibody Campath 1H (6) and the blood anticoagulant Tissue Plasminogen Activator (7).
My team worked on several vaccine candidates including typhoid, tetanus and whooping cough. We were involved in defining the protein pertactin, now part of acellular whooping cough vaccines. Unfortunately, this happened just as the company decided to divest the vaccine business and Pertactin was sold to SmithKline Beecham in a multi-million-pound deal. Clinical trials later proved that pertactin added significantly to the protective efficacy of acellular whooping cough vaccines and so it went on to be licensed as a vaccine component (8). Pertactin is probably the last vaccine antigen discovered in the UK that is now part of a current vaccine (although I am happy to be challenged on this!).
What happened next?
When Wellcome divested from vaccines I stayed on for a couple of years but eventually moved to Imperial College London. I became an academic Professor and established my research laboratory alongside the Medeva R&D. The Medeva team carried on for several years and parts of it went into an Imperial College spin off company called Microscience. Microscience exploited Sequence Tagged Mutagenesis invented by David Holden (9). Eventually the company was acquired by Emergent BioSolutions (https://www.emergentbiosolutions.com) and was moved to the USA. Another opportunity lost to the UK.
In the mid-1990s, Glaxo took over The Wellcome Foundation and the Beckenham site was closed. In 2000, GlaxoWellcome acquired SmithKline Beecham, who had an established vaccine group in Belgium and, unfortunately for the UK, their focus on vaccine discovery and production moved there. It is hard to pin down why GlaxoWellcome and now GSK decided to focus vaccine research and manufacturing outside of the UK, but I assume there were business reasons for doing so. Whatever, Belgium now has a huge GSK vaccine production plant at Wavre (Figure 2) that looks like a small city. This plant, which I have visited, supplies vaccines across Europe. It is reasonable to say that if events had been different this site would have been in the UK. Another opportunity missed?

The changing global picture
During the 1990s the vaccine world changed dramatically, consolidating into a few major vaccine players (GSK, Merck, Pfizer, Sanofi etc) and the ability to manufacture vaccines was lost to many countries. Importantly, it did survive in some including Brazil, Indonesia and Cuba. South Africa also maintained its own capability in procurement but not manufacturing by forming Biovac (//www.biovac.co.za). The UK maintained small vaccine development efforts at Porton Down, focusing on ‘defence vaccines’ and Oxford University (see below) but the decades between 1990-2010 were effectively a vaccine drought in the UK.
A revolution in technology
Just as the UK vaccine industry declined, new technologies opened revolutionary routes to vaccine discovery. Vaccines could now be made for the first time against diseases such as Meningitis B and Hepatitis B. Also, methodologies such as ‘conjugation’ involving chemically linking vaccine components (10) and new adjuvants, which stimulate protection, were invented (11). Leaders in these areas included John Robbins (12) and Rino Rappuoli (13) who headed a new generation of vaccine discoverers.
Inevitably, the UK missed out on this revolution. We did have key players including Richard Moxon and Adrian Hill at Oxford University (14) and David Salisbury (15), who championed vaccines within government (e.g., Meningitis C). I began working internationally with the World Health Organization, Chiron/Novartis and the International Vaccine Institute in South Korea and refocused on building the genomic sciences as Head of Pathogens at the Wellcome Sanger Institute (https://www.sanger.ac.uk).
Seeds of change
A new phase of developments in the vaccine world were driven by the growing acknowledgement that cheaper, cost effective vaccines were needed for those living in the poorer economic nations. The remaining large vaccine companies showed little interest in supplying vaccines into lower- and middle-income countries and vaccine supplies in the most deprived regions fell under threat. Additionally as new vaccines were invented, they were not being passed on into poorer regions.
Partly in response, The WHO created the Expanded Programme on Immunisation (EPI) for common childhood diseases (16). Tore Godal and other global influencers, then created the Global Alliance for Vaccines and Immunisation (https://www.gavi.org), dedicated to providing vaccines to those who could not afford them. This created a market pull for vaccines where one had not existed. Indian entrepreneurs, recognising a business gap, set up companies to make low-cost generic vaccines for the Indian market e.g. Serum Institute of India (https://www.seruminstitute.com) and Biological E (http://www.biologicale.com). Initially, these businesses were largely ignored by western companies, but in time they would grow into power houses in their own right and now challenge the global market. India has an enormous vaccine manufacturing capacity, now proving vital in COVID times.
Then, the Bill & Melinda Gates Foundation (https://www.gatesfoundation.org), declared their intent to champion vaccines for the very poorest. This had an enormous impact and was a game changer, stimulating others to follow. The International Vaccine Institute (IVI, https://www.ivi.int) was formed in South Korea to define the vaccine-targetable disease burden in low-economic countries and develop vaccines that match these requirements (Figure 3). Significantly, locating IVI in Seoul stimulated a fledgling vaccine industry in South Korea.

In the mid 2000s, The Novartis Vaccines Institute for Global Health (NVGH) was established in Siena by Rino Rappuoli as a not-for-profit to make affordable quality vaccines. To create NVGH, a small team (including myself) was formed to develop the concept. Eventually funding was approved, and Allan Saul (17) became the first Director. I also worked as Chair of the Novartis Vaccines Scientific Advisory Board throughout the first decade of this century, witnessing first-hand remarkable developments in vaccinology (see Personal Perspective at end of Blog).
Meanwhile, back in the UK
In the late 2000s, The Wellcome Trust created its own affordable vaccine initiative through their then Chairman Bill Castell (18). In a partnership with Merck, they formed The Hilleman Laboratories (https://www.hillemanlabs.org), in Delhi, India. While I was serving on the Hilleman Board, we introduced the idea of developing a new cholera vaccine, now called Hillcol, created by Jan Holmgren and Michael Lebens in Gothenburg. Hillcol, based on a modified Vibrio cholerae strain known as ‘Hikojima’ (19), is now being developed by Bharat Biotech (https://www.bharatbiotech.com) for licensure at around a dollar a dose.
As the Director of The Wellcome Trust, Jeremy Farrar (20) has acted as a global ambassador for the charity, further developing their international vaccine portfolio. Prior to becoming Director, he worked in Vietnam, where he was involved in the SARS and H1N5/H1N1 flu epidemics personally experiencing the impact of these diseases as a working clinician. During his tenure Wellcome has contributed to the formation of the Coalition for Epidemic Preparedness (CEPI, https://cepi.net). Wellcome also created an in-house priority area for vaccines headed by Charlie Weller (21) and a portfolio of vaccines within their Innovations group, further rejuvenating UK capability and expertise (22).
Where now for the UK (and other countries)?
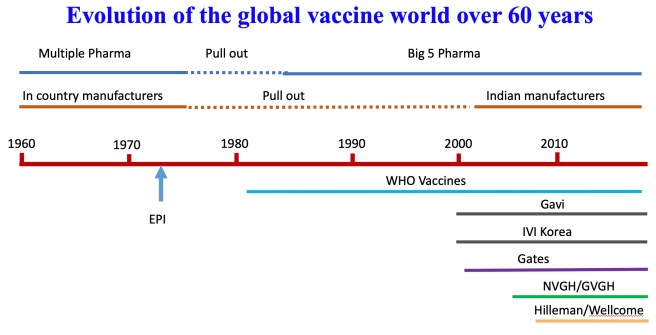
The vaccine world has changed dramatically over the past 50 years (Figure 4, 5). The stimulation provided by the current COVID-19 epidemic is creating a heated debate around national vaccine capacity in the UK and access to vaccines globally. The next steps will be crucial, and clarity of thought and strategic planning will be essential.
The UK has many strengths in vaccinology but currently does not have the complete package. COVID-19 has shown us that with new technologies there will be many opportunities to develop new vaccines in the future (Figure 6). Oxford University has built on the legacy of Richard Moxon, through support for The Jenner Institute (https://www.jenner.ac.uk) and The Oxford Vaccine Group (https://www.ovg.ox.ac.uk). The Jenner Institute was set up by GSK and the BBSRC to reinvigorate UK vaccine science. It was originally based at the Institute for Animal Health in Compton, Berkshire and struggled because of problems with the location and a drift towards basic immunology (23). However, Adrian Hill (24) and others saw the value in not only the name but the scientific mission and rescued it for the UK. This platform has allowed multiple investigators, including Sarah Gilbert, to flourish in a vaccine development-savvy environment. For example, they made tremendous contributions to vaccine development for malaria, ebola and typhoid. This infrastructure and knowhow proved vital to getting the Oxford-AstraZeneca vaccine off the ground so quickly.
The Oxford Vaccine Group has also established a human infection challenge facility that has reduced the time to license vaccines such as typhoid Vi-conjugates (25). I was a co-applicant on Andy Pollard’s Wellcome application to establish a typhoid human challenge capability and there was significant opposition to the concept. However, it turned out to be a game-changer, establishing human challenge on the regulatory path.
Imperial College has developed a vaccine programme through faculty such as Robin Shattock and Peter Openshaw (26, 27). Robin created an RNA-based vaccine system, which is now being developed for COVID-19 and he also runs the UKRI-funded vaccines innovation hub (28). Imperial has also developed human challenge capabilities for respiratory viruses, very valuable for the UK and these may be exploited for COVID-19 (29).
The London School of Hygiene and Tropical Medicine, headed by the renown global health leader Peter Piot (30), is strong in many vaccine related areas including modelling. The UK Manufacturing Hub (https://www.vmicuk.com) has been established and Public Health England (PHE) has retained expertise including at its site in Porton Down (31).
Unfortunately, it will not be easy to bring all of this together overnight and create an effective vaccine machine with all the knowhow integrated into a working system.

Figure 5. Although most vaccines have not been manufactured in the UK for many years new vaccines have been regularly introduced
What to do now?
We now have an opportunity to put the UK (as indeed do other countries and regions) back at the forefront of vaccine discovery, development and manufacturing. We need to do this in partnership with other countries or political groupings while avoiding vaccine nationalism. The UK Vaccine Task Force wisely placed preorders for a variety of different COVID-19 vaccines. Most of these involve at least one of the big vaccine multinationals or Biotech’s. However, most of these vaccines will be initially manufactured overseas, mainly in European countries as the UK rebuilds a manufacturing capacity.
COVID-19 is also providing opportunities to evaluate vaccine approaches that have had relatively little testing in humans e.g. mRNA-based vaccines (11). Ironically many of the larger companies were reluctant to develop disruptive technologies that would fit poorly into their vaccine portfolios. COVID-19 has been a disruptor not only for vaccine companies but also for the regulators.
There has been much talk about vaccine equity since the COVID-19 pandemic, but this is not a new topic. WHO, Gavi and now COVAX (32) will strive to generate the momentum for more equitable COVID-19 vaccine distribution with the hoped knock-on effect for other vaccines. In my view the best way to gain vaccine equity is to get a more equitable global distribution of vaccine knowhow at all (discovery, development, regulation, manufacturing etc) levels. This is particularly true on the African continent, but gaps exist across the globe. Regional development can generate local confidence and production of the vaccine types more appropriate for local populations. Not all infectious diseases are a global threat, so regional vaccine hubs make scientific and ethical sense.
It is perfectly feasible for the UK (and other countries/regions) to redevelop an integrated vaccine industry or support structure outside of the classical pharma model, but will it choose to do this? Unlikely, but here are some thoughts: –
- We need to form regional or country-based vaccine organisations that are impartial, serve the public and understand vaccines from discovery to post-licensing. These are particularly needed in resource poor settings. Such entities should be in public ownership and work with the pharmaceutical industry. They should also be involved in actually making licensed vaccines. They could then work with more centralised systems such as Gavi and WHO.
- Such entities could take a real look at exactly which vaccines, vaccine combinations and immunisation schedules really suite the country and region. One of the criticisms of some anti-vaxxers is that vaccines are in the domain of big business and are driven by profit and not health considerations. This might serve at least to start to address this criticism.
- The whole process of vaccine development from discovery right through to manufacturing, licensing and sales could then be much more joined up locally. This could also drive local scientific innovation, local industries and even bring more public engagement in a positive manner.
- Countries/regions need to bring back the ability to manufacture vaccines at scale. We need to disperse vaccine knowhow and manufacturing across the globe.
- As countries/regions set up their own local manufacturing capabilities links between these will be essential. We need a joined up global vaccine network. This would stop vaccine nationalism and drive collaboration.
- The procurement of vaccines could become much cheaper.
- Large companies want blockbuster vaccines that can generate billions rather than millions of dollars. Regional entities could target those diseases and pathogen types that are regionally common even if the market is smaller. Vaccines would then match regional diseases.
- Some bacterial species are huge and diverse, and it may be better to go after genetic/serological clades, particularly those that are antibiotic resistant or successful in certain cohorts e.g. E. coli ST131. Here clusters of clade-based vaccines linked to regional circulating types may be an option. These could be linked to rapid diagnostics and monoclonals. Smaller regional vaccine entities could champion such approaches that may be less attractive to multi-national companies.
- Adjuvants are a limiting factor for vaccine development. We have few licensed adjuvants that are in the hands of only a few companies. We need to invent new open access adjuvant available to all.
- Countries could decide which market/cohorts to aim for. Would they target epidemics e.g. stockpiling vaccines, or would they compete in other settings e.g. children’s vaccines, combination vaccines?
- Could they specialise in different manufacturing platforms? This would simplify building combination vaccines. Platforms might include vectored vaccines, mRNA vaccines or adjuvanted vaccines. Platforms facilitate combination vaccines if applied to the right diseases.
- Industrial input is absolutely essential, and the role of the global vaccine manufacturer remains central. However, we could build a more open and interactive pre-competitive environment to encourage companies to engage and collaborate.
- How will the future regulatory environment develop post COVID? Countries/regions will need to strengthen their regulatory systems and also build gold standard testing and standardisation centres such as The National Institute for Biological Standards and Control (NIBSC) in the UK (33). NIBSC are world leading in test assays for vaccines. This is key as many vaccines are licensed on correlates approved in part by regulators.
- Could we redesign even the simplest vaccines like tetanus and diphtheria, which are really complex products from another era. Any big pharma would say no or that this is commercially impossible, but a UK market could be innovative and do this. ** They could be the building blocks for a completely new generation of vaccines.
- If we build hubs with integrated vaccine development capabilities all on individual sites, we could bring innovation right through the vaccine pipeline while strengthening industry regionally.

Summary
The COVID-19 pandemic has turned our attention back to the national and regional requirements for vaccine development and procurement. A similar story will play out in different countries across the world. Fortunately, we are now in a unique position to not only reformulate national vaccine programmes but also to take a long hard look at what we really want to use vaccines for and when. We could, for example, completely redesign the current UK vaccination programme. What diseases should we vaccinate against and when? Do we still need to use all of the EPI vaccines or are there other priorities (Figures 5, 6)? It is also an opportunity for an informed public debate, which in the end may bring people closer to understanding both the value of vaccination and the need for a proper risk assessment of the area. This will be needed also to tackle vaccine hesitancy and build public trust.
Personal perspective. I worked as Chair of the Novartis Vaccines Scientific Advisory Board for a decade, witnessing first-hand remarkable developments in vaccinology. Working with Richard Moxon and Mariagrazia Pizza, Rino invented the genomic-based antigen screen ‘Reverse Vaccinology’, which was used to create Bexsero, the new Meningitis B vaccine (34). Importantly, the Siena operation dramatically illustrates how one or two people can make all the difference between success and failure and simultaneously conserve within-country expertise.

*The Wellcome Foundation was a pharmaceutical company formed at the start of the 20th Century. Upon his death, the founder Henry Wellcome’s will directed the formation of The Wellcome Trust who owned the company and used the profits to support scientific research. The Wellcome Trust gradually diversified this asset by selling share in The Wellcome Foundation leading to the sale to GSK in 1995.
** We had a programme in the 1990s to develop purified tetanus and diphtheria vaccines. You may ask why? Well, these vaccines are made of bacterial extracts rather than purified antigens and it might be easier to develop combination vaccines with purer components. Whatever, these are the building blocks of any children’s vaccine programme..
Thanks
I would like to thank Chris Hale and Sophie Palmer for helping me with this blog. And to all others I have worked with in a long career. All the thoughts are my own, as are the mistakes!
Bibliography
- https://www.pnas.org/content/111/34/12288.long
- https://www.nature.com/articles/337709a0
- https://www.independent.co.uk/news/business/news/celltech-merges-with-struggling-medeva-to-create-pound13bn-group-740576.html
- https://www.ncbi.nlm.nih.gov/pubmed/6355363
- https://www.nobelprize.org
- https://en.wikipedia.org/wiki/Alemtuzumab
- https://en.wikipedia.org/wiki/Tissue_plasminogen_activator
- https://www.tandfonline.com/doi/abs/10.1586/14760584.6.1.47?journalCode=ierv20
- https://science.sciencemag.org/content/269/5222/400.long
- https://en.wikipedia.org/wiki/Conjugate_vaccine
- https://gordondougan.blog/2020/04/09/how-to-make-a-new-covid-19-vaccine-starting-from-scratch/
- https://www.sabin.org/sites/sabin.org/files/robbinsmedalspeech.pdf
- https://en.wikipedia.org/wiki/Rino_Rappuoli
- https://www.paediatrics.ox.ac.uk/team/richard-moxon
- https://www.chathamhouse.org/expert/professor-david-salisbury-cb
- https://www.who.int/immunization/programmes_systems/supply_chain/benefits_of_immunization/en/
- https://au.linkedin.com/in/allansaul
- https://en.wikipedia.org/wiki/William_Castell
- https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0108521
- https://en.wikipedia.org/wiki/Jeremy_Farrar
- https://wellcome.ac.uk/about-us/teams/vaccines-team
- https://wellcome.ac.uk/what-we-do/our-work/innovations-flagships
- https://en.wikipedia.org/wiki/Jenner_Institute
- https://en.wikipedia.org/wiki/Adrian_V._S._Hill
- https://www.ovg.ox.ac.uk/team/andrew-pollard
- https://www.imperial.ac.uk/people/r.shattock
- https://www.imperial.ac.uk/people/p.openshaw
- https://gow.epsrc.ukri.org/NGBOViewGrant.aspx?GrantRef=EP/R013764/1
- https://onlinelibrary.wiley.com/doi/full/10.1002/eji.201746942
- https://www.lshtm.ac.uk
- https://www.gov.uk/government/publications/phe-porton
- https://www.gavi.org/covax-facility
- https://www.nibsc.org
- https://www.ema.europa.eu/en/medicines/human/EPAR/bexsero
- http://www.laskerfoundation.org/awards/show/hepatitis-c-replicon-system-and-drug-development/
- http://www.laskerfoundation.org/awards/show/founder-of-molecular-microbial-pathogenesis/
- https://www.tbvi.eu/team/prof-paul-henri-lambert/
- https://www.ae-info.org/ae/Member/Pizza_Mariagrazia
Gordon Dougan FRS is a Professor in the Department of Medicine (https://www.citiid.cam.ac.uk), University of Cambridge and has spent his career leading research into vaccines, pathogen genomics and disease tracking. His research work has helped our understanding of how infections spread around the world, a subject of direct relevance to the current Covid-19 epidemic. He was recipient of the 2020 Albert B Sabin Gold Medal for his work on affordable vaccines and is a Trustee of IVI. This is a personalised version of history. Others may have seen it differently.
